
Download the CVS Challenge Dataset Here!
The SAGES CVS Challenge Dataset

The Data
The SAGES CVS challenge offers a global and diverse dataset of 1000 videos of laparoscopic cholecystectomy procedures, a routinely performed minimally invasive surgical procedure to remove the gallbladder due to inflammation or other pathologies. The dataset was assembled through data contributions from 67 surgeons from 57 countries and 6 continents and encompasses a wide diversity of patient demographics and procedural quality to reflect the worldwide diversity in patients and surgeons. Moreover, the video data is acquired using a variety of laparoscopes from different manufacturers and displays an array of optical properties, which adds to the diversity of the data and ensures adequate representation of the real-world population. The dataset was carefully curated and annotated with respect to the three CVS criteria, following consensus-based protocols incorporating the expertise of worldwide leading clinicians, computer scientists, and industry through structured multidisciplinary Advisory Committees (AC).
CVS Criteria Labels
Each video in the dataset represents a single patient's case, spanning a 90-second segment. This segment starts 90 seconds before one of the relevant anatomic structures composing the CVS (cystic duct or artery) is clipped ("point of no return"). Within each video (90-second segment), additional frames are extracted at five-second intervals (= 18 frames per video) to provide additional training data.
The three criteria defining the CVS are annotated as binary labels (criterion achieved yes / no) for each video and each of the 18 frames per case. No semantic segmentation labels are provided. Moreover, we provide an overall rating of the annotation difficulty for each video, reflecting the annotators' subjective assessment. This does not reflect the surgical/operative difficulty of the case. The annotation complexity is provided as a 0-1 value, representing the annotator's confidence ( 0 = very difficult to annotate/ not confident at all; 1 = very easy to annotate/ very confident). For each video, we provide annotations:
Per Video (Were the 3 CVS criteria achieved in the overall video? Yes / No) = 3 Binary Labels x 3 annotators
Per Frame (Were the 3 CVS criteria achieved in this frame? Yes / No) = 3 Binary Labels x 18 Frames x 3 annotators
Annotation Confidence (How sure was the annotation of the 3 CVS criteria for this case? 0-1 / not confident-confident) = 1 probabilistic label x 3 annotators

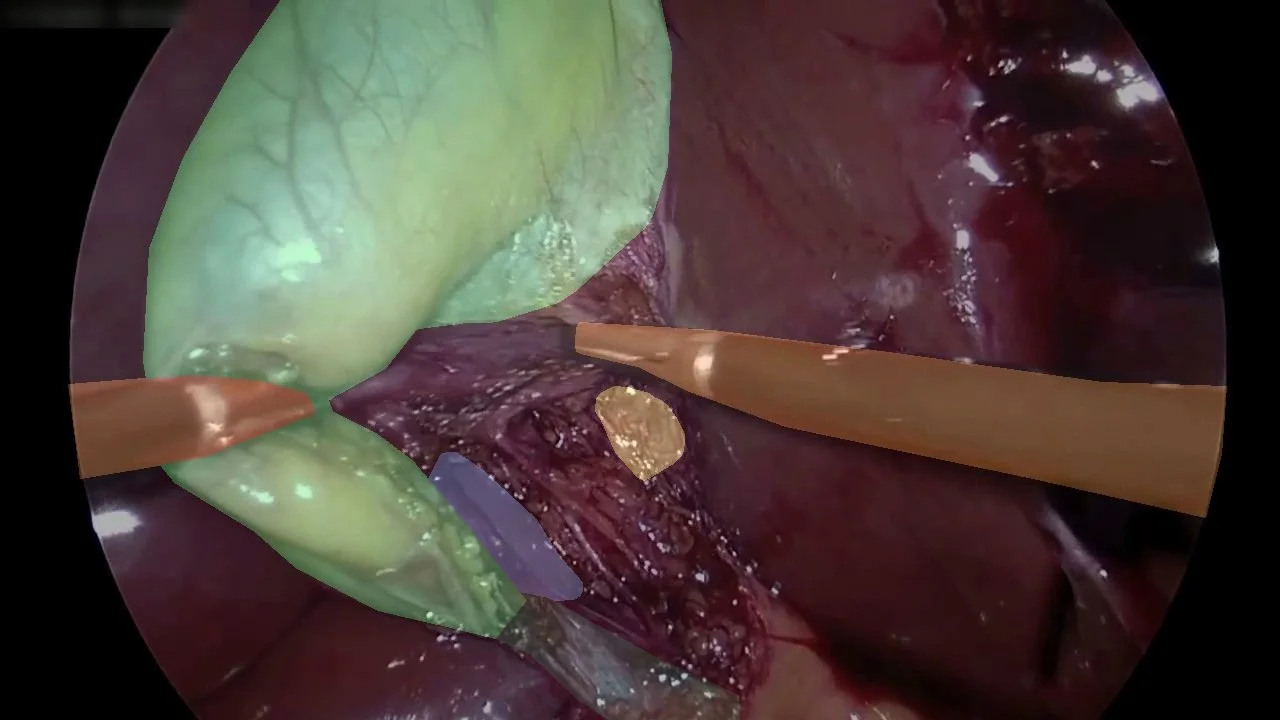
Segmentation Labels (NEW in 2025)
This year, we additionally provide segmentation masks of 5 key hepatocystic anatomical structures and tools. The annotations were collected in a multi-stage process ensuring that each frame was reviewed by multiple expert annotators. A couple example images are provided below.


The Metadata
In addition to the labels described above (per video / per frame / annotation difficulty), we also provide demographic and selected clinical metadata.
Country of data origin (anonymized) = the dataset was composed with contributions from 6 continents, to preserve data privacy the country name is anonymized
Laparoscope Type (category) = The type and manufacturer with which the video was recorded, which can influence the resolution, is provided in pseudonymized categories.
Robotic Surgery (yes/no) = If the video was performed robotically (as opposed to conventional laparoscopy) is provided as a binary (yes/no) label.
Indocyanine Green (ICG) Use (yes/no) = During any laparoscopic cholecystectomy procedure, ICG can be used to better visualize and identify the relevant anatomy under fluorescent light. While ICG is routinely used in some institutions, in others, surgeons might selectively opt to use ICG for an enhanced overview of the operative field. In this case, ICG may indirectly indicate a more difficult case. While you may not see ICG or fluorescence in the provided 90-second video, the label indicates whether it was applied throughout the case.
Intraoperative Cholangiography (IOC) (yes/no) = An intraoperative cholangiography is a measure to visualize the anatomy of the biliary ducts more clearly. During an IOC, the surgeon opens the structure identified as the cystic duct and introduces a catheter into the common bile duct for drainage or to inject dye. This can improve the understanding of the anatomic relations of the structures (cystic duct vs common bile duct) to each other and help to prevent accidental clipping of the common bile duct. Usually, an IOC indicates a more complex case (i.e., due to the clinical history of the patient, complex anatomy, an increased degree of inflammation of the gallbladder). Similarly to ICG, the IOC may be performed outside the 90-second video segment.
Disclaimer: The SAGES CVS Challenge Dataset is currently ONLY accessible to teams officially registered for the MICCAI 2025 CVS Lighthouse Challenge. The dataset should be used solely for the purpose of competing in the official CVS challenge (not for any other academic or commercial purposes). For questions please feel free to reach out to sagescvschallenge2025@gmail.com!